Overcoming Difficult Challenges: The Unique Value Of Menghini Needle in The Diagnosis Of Autoimmune Pancreatitis And Fibrotic Pancreatic Lesions
Apr 30, 2026
In the diagnostic spectrum of pancreatic solid lesions, there are some "difficult cases" that both endoscopists and pathologists find particularly challenging. Among them, autoimmune pancreatitis and focal chronic pancreatitis (especially the type that forms masses) are typical representatives. They often overlap with the imaging manifestations of pancreatic cancer, but the treatment strategies are vastly different. A clear diagnosis is highly dependent on obtaining specimens with characteristic histological changes. However, these lesions are often tough in texture and rich in fibrous tissue, and conventional biopsy needles are difficult to obtain sufficient and high-quality tissue strips. In these challenging scenarios, the Menghini needle, which inherits the essence of the classic liver biopsy needle design, with its "inward-angled cutting and negative pressure extraction" feature, may demonstrate unique value beyond other needle types and become a powerful tool to overcome these diagnostic labyrinth.
I. Diagnostic Challenges: Why Are AIP and Fibrotic Lesions Considered "Biopsy Difficulties"?
1. Autoimmune pancreatitis: The gold standard for diagnosis is histopathology. The core features include: reticular fibrosis, infiltration of lymphocytes and plasma cells (especially IgG4-positive plasma cells), and occlusive venulitis. These features can only be clearly identified in a well-preserved tissue section with sufficient spatial structure. Traditional fine-needle aspiration (FNA) often yields loose cell clusters that are almost impossible to assess for fibrosis patterns and vascular lesions, resulting in an extremely low diagnostic rate (reported to be lower than 10% in literature). Even with early FNB needles, it is often difficult to obtain ideal assessment specimens due to tissue compression and fragmentation.
2. Focal chronic pancreatitis/fibrotic mass: Long-term inflammation leads to extensive replacement of pancreatic tissue by dense collagen fibers, resulting in a leather-like texture. The resistance during puncture is extremely high, and the common needle tip is prone to slipping or bending. The obtained specimens are often small amounts of fibrous fragments, which are difficult to distinguish from the connective tissue hyperplasia reaction of pancreatic cancer, making the diagnosis extremely challenging.
Common challenge: These lesions present nearly contradictory requirements for the biopsy needle - it needs to be able to forcefully penetrate the tough tissue while also being able to gently obtain a complete structure. A needle that solely focuses on "cutting power" may cause tissue pulverization; while a needle with insufficient strength simply cannot obtain an effective sample.
II. How did the design of the Menghini needle respond to this challenge?
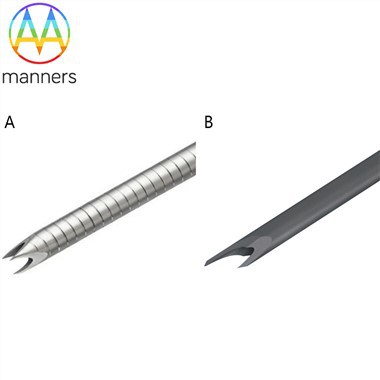
The "inwardly inclined" design of the Menghini needle offers a clever solution at both the physical and physiological levels for dealing with fibrotic lesions:
1. Low-resistance puncture, efficient breakthrough of the fibrous barrier: The inward-sloping surface forms a more sharply pointed "cone tip" in physics. Under the same thrust force, its pressure is greater, enabling easier puncturing of the dense fibrous capsule and access to the lesion core. This reduces tissue compression and needle oscillation during the puncture process, improving the success rate of a single puncture on a hard target.
2. "Picking up" rather than "tearing", preserving the tissue structure: This is the core of Menghini needle's potential advantage. Once the needle tip enters the lesion, the simultaneous negative pressure is not used to "crush" the tissue, but to "gently introduce" the cylindrical tissue in front of the needle tip into the needle groove. The cutting edge of the inward-sloping surface then completes the cutting. Compared to "hooking" (Fork needle) or "rotational cutting" (Franseen needle) from multiple sides, this process may have less shear stress and compression force on the tissue strips. The goal is to obtain a relatively complete "microscopic tissue column" with better cell interconnections.
3. Specimen morphology is more conducive to pathological assessment: Theoretically, the tissue strips obtained in this way can better preserve the internal fiber orientation, vascular structure, and distribution pattern of inflammatory cells. This is crucial for pathologists to identify the characteristic "sheet-like fibrosis" and "occlusive venous inflammation" of AIP. A complete, undistorted tissue strip can also ensure the accuracy and representativeness of immunohistochemical staining (such as IgG4, IgG count).
III. Evidence and Outlook: The Role of Menghini Needles in AIP Diagnosis
Although the existing literature has not conducted large-scale direct comparisons of the advantages and disadvantages of the Menghini needle versus other needle types in the diagnosis of AIP, it has provided important clues and reasoning foundations.
* The benchmark performance of the Franseen needle: A Japanese multi-center prospective study specifically using the 22G Franseen needle for the diagnosis of AIP showed that the overall histological detection rate was as high as 92.7%, and the rate for type 1 AIP reached 58.2%, which was much higher than the historical data using FNA needles. This clearly demonstrates that the new FNB needle capable of obtaining high-quality core tissue strips is a significant advancement in the diagnosis of AIP.
* The potential inference of the Menghini needle: The success of the Franseen needle lies in its ability to obtain sufficient tissue for assessment. If the Menghini needle, with its "tissue structure preservation" advantage, can obtain the same amount or slightly less tissue while providing better structural quality, then its efficacy in the diagnosis of AIP will be highly anticipated. Especially for cases with difficult differential diagnosis, a high-quality tissue strip that clearly shows the fibrotic pattern may have a diagnostic value greater than multiple structurally fragmented specimens.
In the diagnosis of focal chronic pancreatitis, the situation is similar. The efficient puncture ability of the Menghini needle helps to enter the fibrotic mass, and its relatively "gentle" cutting method may obtain complex tissue fragments containing acinar atrophy, duct deformation, fibrous hyperplasia and inflammatory cells, which is more conducive to the pathologist's judgment of "benign hyperplasia" rather than "cancerous connective tissue hyperplasia".
IV. Clinical Decision: When should Menghini needles be considered for use?
Based on the above analysis, in the following clinical scenarios, the operator can give priority consideration to or choose the Menghini needle:
1. When AIP is highly clinically suspected: When the patient has elevated IgG4 levels, involvement of other organs, and characteristic imaging manifestations (the "sausage sign"), to obtain definitive pathological evidence, a needle type with strong tissue preservation ability can be selected. The Menghini needle is a reasonable option.
2. When the histological assessment after routine puncture is unsatisfactory: If the specimens obtained using other needle types are analyzed by the pathology department and they report "excessive tissue compression, unclear structure, and inability to assess fibrosis", switching to the Menghini needle during a second biopsy might be a solution.
3. When the texture of the lesion is abnormally hard under EUS: When the ultrasound endoscopy detects that the texture of the lesion is extremely tough and it is predicted that puncture will be difficult, choosing the Menghini needle with less puncture resistance might increase the success rate of the first puncture.
Conclusion: The precise tools for tackling "difficult problems"
In the arsenal for diagnosing pancreatic diseases, we need "heavy artillery" to break through the defenses of most tumors (such as the Franseen needle with high acquisition capacity), and we also need "precise surgical knives" to dissect the most complex pathological structures. The Menghini needle is precisely such a precise surgical knife. It may not be the needle with the largest "quantity" of tissue acquisition, but its unique design philosophy enables it to have extraordinary potential in obtaining high-quality and assessable "quality" when tackling diagnostic "hard nuts" such as autoimmune pancreatitis and fibrotic masses. In the era of precision medicine, the depth of diagnosis often depends on the quality of the specimen rather than just the quantity. Therefore, when dealing with the most complex diagnostic challenges of the pancreas, the value of the Menghini needle lies not only in being a tool, but also in representing a pursuit of ultimate tissue preservation and a pathology-oriented, refined biopsy strategy.